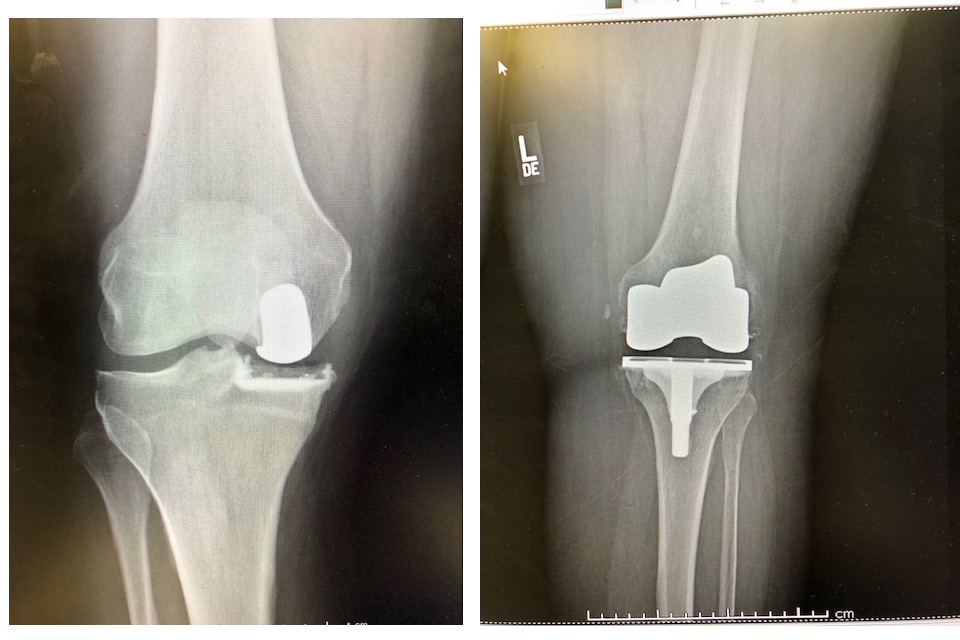
Total knee vs MIPKR
| MIPKR | Total Knee ReplacementMIPKR |
| 3 – 4 inch incision | 8 – 9 inch incision |
| Quadriceps muscle not cut, kneecap not dislocated | Quadriceps muscle cut and kneecap turned over and dislocated |
| ACL and PCL left in place to stabilize knee | ACL and usually PCL (stabilizing knee ligaments) removed |
| very little bone removed | large amount of bone removed |
| very little blood loss | significant blood loss |
| formal therapy usually not needed, patients exercise on own | formal physical therapy required average about 2 months |
| walker about 3 days, cane a week* | walker 2-3 weeks, cane another 2-3 weeks* |
| narcotic pain meds 3-7 days* | narcotic pain meds 2-4 weeks* |
| infection rate 1 per thousand | infection rate about 15 per thousand |
| antibiotics not required for dental procedures | antibiotics required for dental procedures |
| natural gait | gait permanently altered (to a small degree) |
* There is great variation among patients, these are general observations I have made


Why would anyone choose Total Knee that has unicompartmental OA?
If they are given the choice it is rare for a patient to do so, but the reasons would be:
- Since all of the compartments are resurfaced, the possibility of progression of OA to other compartments is not there. Fortunately this does not occur frequently with partial knees
- There are lots of long term studies that show good durability of total knees, fewer studies long term on partial knees, although mid term studies like my own look promising
- In the presence of morbid obesity a total knee spreads out the weight bearing surface to a larger area and might be a better choice. This has not been proven though
